Published monthly for CC employees by Clinical Center Communications
February 1998
New program
Senator visits
CFC succeeds
Mock ups up
Work life council
King: the legacy continues
Washing hands
Briefs
< |
|

CRC design meetings
continue
"We really want input to make this as functional as possible,"
said CC Director John Gallin at a patient orientation meeting late last
month. CC patients are involved in the design of the patient-care units
for the new facility. Dr. Gallin is shown discussing suggestions with several
patients.
Patients help design CRC
"There are many things from the eyes of a patient that we need to
know," said CC Director John Gallin, during an orientation meeting
for patients held late last month.
Several CC patients, past and present, were invited guests at the meeting,
held to elicit input on the design of the new Mark O. Hatfield Clinical
Research Center.
During the meeting, Dr. Gallin described some of the major accomplishments
that have taken place at the NIH, including the development of the first
treatment for cancer and AIDS. But, Dr. Gallin pointed out, more importantly,
the CC has been a facility committed to the patients.
"We consider the patients truly partners in what we do," he
said. "Without the patients, this place wouldn't exist."
According to Dr. Gallin, several factors necessitated the creation of
a new facility, including the 1940s design of the ventilation and water
systems in the current building, which are nearing the end of their lifespan.
"We said to the architects who were designing the new facility,
please give us a building that can change," said Dr. Gallin.
The new facility, according to Margie DeBolt, architect with Zimmer,
Gunsul, Frasca Partnership, will include interstitial space between each
floor, which will house the mechanical systems. In the current building,
the mechanical systems are hard for technicians to reach and often interrupt
the flow of work in the area if repairs are needed. "The new design
will be a mechanic's dream," she said.
A series of meetings have been conducted to date. They have included
patients and representatives from institutes in an effort to assist with
the design of the labs as well as the patient-care units. Planners stressed
the importance of obtaining input early in the process in order to save
time and money. Patients were encouraged to attend patient-care unit standardization
meetings, which include discussions concerning the design of the units.
"Before we build 250 patient rooms, we would like to get the right
design and duplicate it," said DeBolt.
index
|

Staff on the 4 West Unit include (front row, left to right): Lynn Compton,
Lenora Jones, Sandra Bowles, Bernie Crago, Tammy Daley, and Gerald Hodges.
In back from left are Stefano Marenco, M.D., Tony Santucci, Annie Gilchrist,
Jim Hoagland, Juliaphine Campbell, Lisa Misra, Luella Clausnitzer, Ayman
Bakey, M.D., Agnes Plante, Lucy Justement, Gail Butterworth, and Ben Kosiorowski.
NIMH brings brain disorder clinical program to the CC
The Clinical Brain Disorder research program of the NIMH, previously
carried out at the William A. White Neuroscience Center on the grounds of
St. Elizabeth's Hospital in Washington, D.C., has moved to the Clinical
Center.
The 4 West patient-care unit now headquarters this research program on
schizophrenia and other serious mental illnesses.
"The Intramural Research Program Planning Committee last year recommended
relocating the Center to the Bethesda campus in order to preserve the best
elements of this remarkable program," said Dr. Susan Swedo, acting
scientific director, NIMH. "The NIH campus provides the services identified
by the committee, which include access to imaging facilities, collaboration
and training opportunities, and enhanced patient access. Cost savings were
also a consideration."
Under the first phase of the relocation, the CC nursing staff designed
orientation activities for patients and staff. "This relocation was
a major integration that required major planning," said Jacques Bolle,
chief of the mental health, alcohol, and aging nursing services, CC nursing
department. "The CC nursing staff was very involved early on by planning
visits from St. Elizabeth's patients and staff to orientate them to the
unit setting and the various departments in the CC."
The unit received structural and staff changes to accommodate the additional
patients and personnel. To date, seven patients have been added to the unit,
with more slated to be added in coming months. In addition, more than ten
patient-related staff were moved from St. Elizabeth's to the Clinical Center.
"This move had an impact on the professional and personal lives of
many staff, St. Elizabeth's as well as CC," said Bolle. "It shows
the team effort among these groups as theystrive for excellence in patient
care."
"The relocation is a great example of collaboration among the institutes,
as well as the NIH and CC staff," said Dr. David Henderson, CC deputy
director for clinical care. "Everyone together did a remarkable job
preparing for the transfer."(by LaTonya Kittles)
index |

Senatorial visit
Senator Mike DeWine (R-Ohio), a staunch supporter of legislation for
pediatric research, recently visited several patients on 11 East. During
his visit DeWine also met with several institute physicians to discuss issues
relating to children's research at NIH, including asthma, mental health,
and cancer. Shown (left to right) are DeWine, Dr. Jack Yanovski, pediatric
unit ward chief, and CC patient Nicholas Narlock.

Mock-ups going up
Mock-ups of patient rooms in the new Clinical Research Center will be
used as a planning tool by the design team and the various NIH planning
groups over the next few months. The rooms will take shape to reflect design
refinements. Shown is the first step of the project, located in the 14th
floor assembly hall. |
|
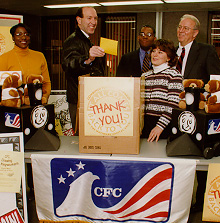
CFC succeeds
The Clinical Center exceeded its $90,000 goal during the CFC campaign,
with total contributions from NIH topping well over $1.5 million. During
a CFC raffle last month, program planners picked names for keyworker and
contributor prizes.
Awards for CFC contributors were: First prize, two airline tickets, to
Robert Wesley, NCI; and second prize, a 20-inch television, to Paul Russell,
NEI.
Keyworker awards were: First prize, two airline tickets, to Cordell White,
Jr., NEI; and second prize, a $100 Montgomery Mall gift certificate, to
Joan Kraft, NINDS.
Shown are (left to right) Diedre Andrews, CC; Dennis Askwith, NHLBI;
Walter Jones, CC deputy director for management and operations; Randy Schools,
R&W; and Karen Ciaschi, R&W. NIH keyworkers will be recognized for
their hard work and contributions during a ceremony in March.
index |
CC council to examine issues of working life
The CC Quality of Worklife Initiative (QWI) Council,
designed to explore issues affecting employee work life and propose options
for improvements, met for the first time on January 30. The Council is an
important component of the CC Quality of Worklife Program.
"We plan to work towards accomplishing goals set forth by both the
HHS and NIH Quality of Worklife Initiative programs, which include improving
employee satisfaction, strengthening workplace learning, and helping employees
better manage changes when they occur," said Walter Jones, CC deputy
director for management and operations. "The Council will also be charged
with further exploring issues that are unique to CC employees."
The diverse Council consists of twelve members representing a cross-section
of Clinical Center employees. Plans for the first year include exploring
issues of importance to employees through departmental surveys, collaborating
with NIH and HHS QWI groups on pertinent programs, and tracking and monitoring
implementation of action items.
"We anticipate that the Council will serve as a resource to CC staff
by obtaining and sharing information on family- and employee-friendly programs
and opportunities," said Jones.
index |

Martin Luther King, III was keynote speaker for January's
NIH prgram honoring the contributions of Martin Luther King, Jr. |

Walter Jones, CC deputy director for management and operations
(right), greets King after the Jan. 16 program. |

The Aurora Dance Company presented a spiritual dance, "Songs
of Sorrow and Jubilee," as a special tribute. |

The Cardozo Hight School choir entertained. |
The legacy continues: Martin Luther King III commemorates his father's
life, times, and dreams
There was standing room only. By quarter past the hour, all seats in
Masur Auditorium were filled. Latecomers were ushered to the visitor information
center or the 14th floor auditorium. Closed circuit coverage was their only
solace. And, oddly enough, even though they were not physically present
in the auditorium, they could still feel the aura, the inspiration of a
room filled with people set to praise not only the memory of a slain leader,
but the legacy for which he gave his life.
They had all come on January 16 to participate in a commemorative program
observing the life and legacy of Dr. Martin Luther King, Jr.
Music and self-expression marked the ceremony, as youth from Cardozo
High School and the Aurora Dance Company communicated with their voices
and their movement, paying tribute to Dr. King. With every note and sway
of their bodies, their message was clear: The power of a body of individuals
who believe spiritually can overcome all of life's struggles. As the keynote
speaker said, "Prayer changes things."
Martin Luther King, III, the second oldest of the four children of Dr.
Martin Luther King, Jr., and Coretta Scott King, had just one day before
become president of the Southern Christian Leadership Conference, co-founded
by his father in 1957. And as he discussed his hectic travels during the
week preceding his visit to NIH, he said, "If there was any place that
I was going to collapse, this [NIH] would be all right."
As King discussed his father's dreams and aspirations for the future,
he said that he felt our society has fallen short of expectations set years
ago. "His message was so simple, but we still haven't gotten it right.
We are the most resourceful nation on this planet, yet we continue to suffer
from the most disabling disease of all-that disease of racism. Over three
decades ago, Martin Luther King, Jr., depicted racism as America's greatest
moral dilemma, and 30 years later, it is still our greatest moral dilemma,"
said King. "One that has the potential to consume and destroy us, if
we continue to legislate, adjudicate, allocate, and educate in a divisive
and discriminatory manner."
King said the society that his father preached about having one day,
in which his children were judged by the content of their character, rather
than the color of their skin, has yet to be achieved. "There are those
who will have you believe that in 1998, 30 years after the assassination
of my father, we now live in a color-blind, gender-blind, age-blind, class-blind
and disability-blind society," he said. "Perhaps they are so blind
they cannot see the sobering reality around us."
Discriminatory practices by corporations, lending institutions, and workplaces
have, according to King, kept that dream from becoming a reality. "We
need only look in our nation's boardrooms to see that that day about which
my father spoke is not today." He urged participants to assess their
own workplaces. "You must evaluate if it is today at NIH; that is your
job," he said.
According to King, problems in our society, among all races, are not
adequately addressed. "W.E.B. Dubois taught it's easy to make people
with problems, problem people," he said. "Once we decide a group
of people are problem people, its easy to dismiss them and their problems."
For example, he said, "It's easy for many to overlook the disproportionately
high incidence of death and disease among minorities in our nation. When
we decide that a group of people are problem people, then we don't really
have to examine the root of the problem."
But King suggested moving beyond that by viewing the needs of a society
as a whole. "We have to address the issue of all of God's children
who are suffering in America." he said. In discussing what King calls
the "color game," he said that people often link problems to a
specific group, rather than making them a societal problem. "When we
talk about the problems of affirmative action, we talk about the alleged
black student who took the place of the white student, not the discrimination
of the white female who has benefited most from affirmative action,"
he said. "When we talk about the drug problem, we don't discuss the
wealthy white businessman doing lines of cocaine before a Wall Street meeting,
or the wealthy white female who does lines of cocaine before her tennis
match; rather you see the face of a young hip-hop, hat-to-back-worn young
black man."
He also cited inconsistencies in the English language, which associate
black with things that have bad qualities, as well as the tendency of the
media to disproportionately show people of color in a negative light.
"I bring all this to your attention because if we stop perpetuating
the things that divide us and start acknowledging the things that link us,
then we can move towards realizing the dream of my father." He added,
"Martin Luther King's dream was an American dream, not an African-American
dream."
Although he said that we fall short of the dream, he does feel that there
is hope, especially at NIH. "For [here at NIH] there appears to be
a commitment to advancing the dream of equality and freedom from human illnesses."
King noted the importance of the Office of Research on Minority Health and
encouraged individuals to not only continue their focus on fighting death
and disease among minority populations, but also to increase minority participation
in the conduct of research, despite ills that have been done in the past.
"We must proceed cautiously and understand that there are some good
people who are trying to do good work and we must becoEncouraging the NIH
to increase the number of physicians of color, King stated the importance
of their inclusion in the process. "There are brilliant scientific
minds out there who happen to be minorities," he said. "Here [at
NIH] where you have over 1,200 tenured scientists, and I think eight are
African American. I want to encourage you to work on that number,"
he said."Not to be and to say something negative, but we must do better,
we've got to do better, and mostly, we can do better." (by LaTonya
Kittles)
index |
Handwashing:
as important today as it was yesterday
|
 |
A contest: The CC Hospital Epidemiology Service
is looking for a slogan to complement new artwork for a handwashing campaign.
Rules: The slogan must be brief, concise, and capture the importance
of handwashing on a regular basis.
How to enter: The entry form for submission is available on the HES web site, at http://www.cc.nih.gov/hes. Suggestions can be sent via interoffice mail to
HES, Building 10, Room 4A21, or e-mailed to abooze@pop.cc.nih.gov.
The deadline for submission is February 20, 1998.
OR
Visit the "handwashing booth" outside the B1 cafeteria from
February 16-20 and drop your suggestion in the box.
Winners will receive a $15 gift certificate from Blockbuster Video and
be highlighted in an upcoming issue of the CC News. |
Did you know?
- Handwashing is the first line of defense against many diseases, such
as the common cold.
- One in four food-borne illnesses result from poor hygiene, generally
unwashed, or poorly washed hands.
- The Centers for Disease Control and Prevention calls handwashing the
"single most important means of preventing the spread of infection"
from bacteria, pathogens, and viruses.
- In general, health-care workers wash their hands only about 50 percent
of the times they should.
- If you don't wash your hands, you are more likely to have germs that
can be infect yourself and others.
For more than a century, we have known that infectious agents can be
spread by the hands. Many items that we touch everyday can carry viral and
bacterial organisms left by someone who did not wash their hands. The potential
modes of organism transmission include touching the inside doorknob of a
public bathroom, putting your mouth to the receiver of a public telephone,
preparing raw meats in the kitchen, changing a diaper, grasping the handle
of a supermarket cart, or shaking hands with someone who just covered their
mouth while sneezing.
Unfortunately, we can't avoid all these objects and activities, but we
can wash our hands often and not touch our mouth, eyes, or nose until we
have.
In essence, frequent handwashing is a major cornerstone of infection
protection and health promotion for all persons.
Handwashing works by removing organisms that are acquired from infected
persons or contaminated objects. Individuals should wash their hands when
visible contamination or soiling occurs, after using the bathroom, changing
a diaper, handling money, blowing your nose, sneezing, or coughing, handling
a pet, taking out the garbage, handling any body fluids, tending persons
with known infections, and before and after eating, feeding, or handling
food.
For health-care workers, washing hands is an important part of infection
control. Hands should be washed both before and after direct patient contact,
after contact with blood or other potentially infectious materials, such
as equipment or articles contaminated by blood, and after removal of gloves
or other personal protective barrier equipment.
Three elements are essential for good handwashing: soap, running water,
and friction.
Here are some tips:
- Be certain to use a rubbing action that creates a lather over the entire
hand surface.
- Wash all surfaces of the hands and fingers for 10 to 15 seconds, then
fully rinse with running water.
- If possible, turn off the faucet with a paper towel.
- Dry hands with disposable or single-use towels or an air-dryer.
Numerous non-antimicrobial and antimicrobial handwashing products are
currently on the market. These products can be purchased in numerous forms,
including: bar, liquid, premoistened towelettes or wipes, granule, powder,
leaflet, or soap-impregnated tissues. Non-antimicrobial soap works by suspending
microorganisms, allowing for their mechanical removal. On the other hand,
antimicrobial, or antiseptic agents are products with germ-killing activity
designed for use on skin.
One of these agents, triclosan, is found in many antibacterial soap products
available in many grocery and convenience stores. Another agent, chlorhexidine
gluconate, is used in various patient-care areas in the Clinical Center,
such as the ICUs. If you do not have immediate access to a sink, there are
other ways to kill germs. Waterless handwashing products are also readily
available on the market.
The CC uses a multi-factored approach to help promote handwashing. Staff
have access to supplies that are convenient and easy-to-use. Additional
supplies are available by calling the Housekeeping and Fabric Care Department
at 6-2417.
CC staff also receive training concerning infection-control practices
through the Universal Precautions training, as well as other programs. The
CC develops educational programs and campaigns designed to communicate the
importance of handwashing.
In an effort to change with the times, the current handwashing sign "washing
hands prevents infection," which can be found in all CC public restrooms,
will be updated. We invite you to participate in our CC-wide contest to
develop a fresh slogan to complement newly designed artwork. The ideal slogan
will be short and clear in meaning. All entries must be received between
February 9 and 20, 1998. Entries may be submitted outside the B1 cafeteria
during the week of February 16, mailed to HES, Bldg. 10, Room 4A21, faxed
to 6-0457, or e-mailed to abooze@pop.cc.nih.gov.
The winning entry will become the new CC handwashing slogan. The winner
will receive a $15 gift certificate to Blockbuster Video, and their picture
and slogan will be displayed in an upcoming CC News. (by Annette
Booze and Barbara Fahey, Hospital Epidemiology Services)
index |
News briefs
For the latest news about confidentiality of patient information at the
Clinical Center, visit the Confidentiality Education Group (CEG) website,
http://www.cc.nih.gov/ccc/ceg/
Weather alert
Although this year's winter has been quite mild, remember that the threat
of bad weather isn't over yet. Weather policy, including your emergency
employee status, is important to know before a storm hits. For more information
on your status-and what you're supposed to do when ice and snow close down
the government, speak to your supervisor.
CC board holds first meeting of the year
The CC Board of Governors held its first meeting of 1998 on January 23.
Discussions included updates on the strategic plan as well as the new CC
budget process, and highlights from the 1997 annual report. |
Benefit statements coming this month
Last year, for the first time, the Office of Human Resources Management
(OHRM) provided all CC employees with an employee benefits statement. After
a favorable response from employees, the OHRM will once again mail all employees
their individual summary of benefits and compensations. Enclosed in your
packet this year will be a customer satisfaction survey to share ideas and
comments with the OHRM personnel operations section. Look for your statements
in the mail soon. If you have any questions or comments, call Sharon Reed
at 6-6924.
Training offered
Learn the basic skills needed to deliver a presentation by attending
"Getting Up to Speak" on February 25 from 8:30 a.m. to 4:30 p.m
in the first floor conference room at 6100 Executive Blvd. To register or
for more information, call the education and training section at 6-1618.
Events to celebrate
In honor of African American History Month, which is February, all NIH
cafeterias run by Guest Services will showcase tasty, heart-healthy African
American dishes from the NHLBI "Stay Young at Heart Program."
Throughout the month, those who buy a featured diet at a cafeteria will
receive a special heart-healthy gift. The NHLBI hopes the program will show
how easily traditional recipes can be made healthier without losing any
of their taste.The showcased recipes have been compiled in a new NHLBI publication,"Heart
Healthy Home Cooking, African American Style," available from the R&W
for $2.50.
index |
| Clinical Center News, 6100
Executive Blvd., Suite 3C01, MSC 7511, National Institutes of Health, Bethesda,
Maryland 20892-7511. (301) 496-2563. Fax: 402-2984. Published monthly for
CC employees by the Office of Clinical Center Communications, Colleen Henrichsen,
chief. News, articles ideas, calendar events, letters, and photographs are
welcome. Deadline for submission is the second Monday of each month. |
Editor: LaTonya
Kittles
top | cc home page
| nih home page | |
|

